The Historical Evolution of Pain Concepts: From Mysticism to the Biopsychosocial Model
1. Introduction
Pain has been an intrinsic part of the human condition since the earliest stages of human history and remains among the most frequent reasons for seeking medical care. Despite its ubiquity, pain has long resisted precise definition, comprehensive explanation, and effective treatment. Its interpretation has evolved alongside advances in scientific knowledge, while also reflecting broader cultural, philosophical, and societal influences. The history of pain is therefore not merely a medical narrative, but a reflection of how humans have sought to understand suffering, the body, and the mind.
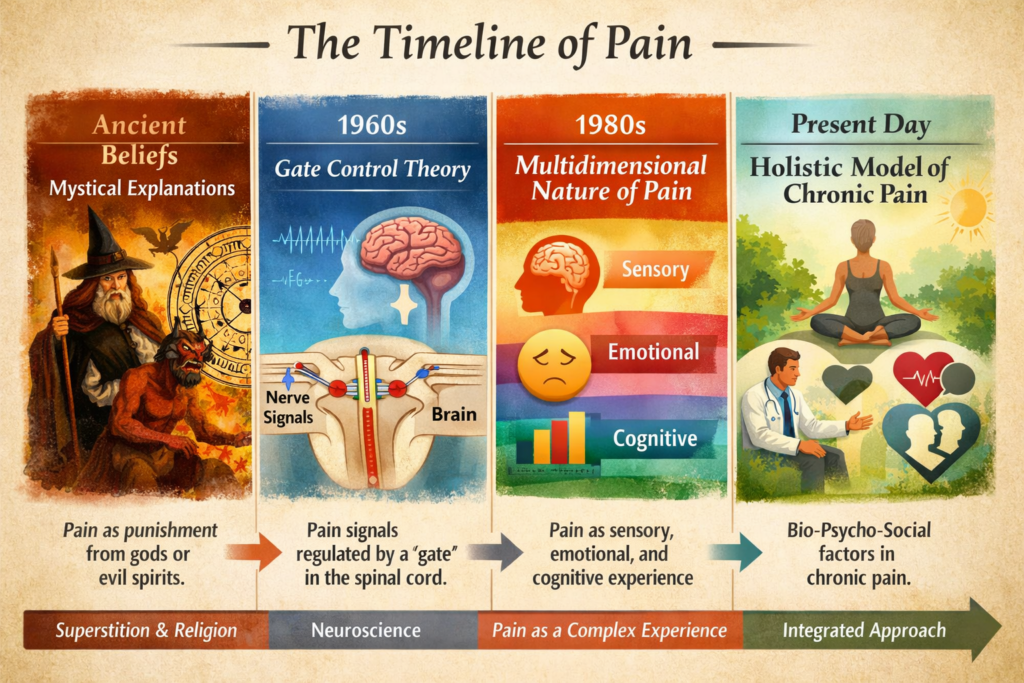
Examining the evolution of pain theories is essential for understanding contemporary pain medicine, which increasingly recognizes pain as a complex, multidimensional experience rather than a purely sensory phenomenon. This review presents a chronological overview of major historical concepts of pain, ranging from early mystical and spiritual explanations to modern biopsychosocial models. Particular emphasis is placed on the development of neurophysiological theories, the growing recognition of psychological processes, and the eventual incorporation of social and contextual factors into current pain frameworks.
2. Pain in Antiquity: Spiritual and Natural Explanations
2.1 Early Civilizations and Analgesic Practices
The earliest documented approaches to pain date back more than 5,000 years. Clay tablets from Mesopotamia describe the cultivation of opium poppies, indicating early recognition of pain-relieving substances. In ancient Egypt, opium poppies were found in burial tombs, suggesting both medicinal and ritualistic uses. These early practices demonstrate that pain relief was intertwined with natural elements and spiritual beliefs.
(https://www.timesofisrael.com/israeli-archaeologist-uncovers-earliest-known-use-of-opium-in-the-ancient-world/)
2.2 Greek Philosophy and Medicine
Greek thinkers laid the foundation for Western medical thought. Homer’s Odyssey describes the use of opium to alleviate sorrow and pain, illustrating an early understanding of pain as both physical and emotional. Aristotle, however, did not classify pain as a sensory modality. Instead, he considered pain and pleasure to be emotions or “passions of the soul,” often caused by external disturbances such as evil spirits entering the body through wounds.
Hippocrates introduced a more naturalistic explanation, proposing that pain resulted from an imbalance of the four bodily humors. Notably, the brain was not considered central to pain perception; instead, the heart was viewed as the seat of sensation. These ideas dominated medical thinking for centuries.
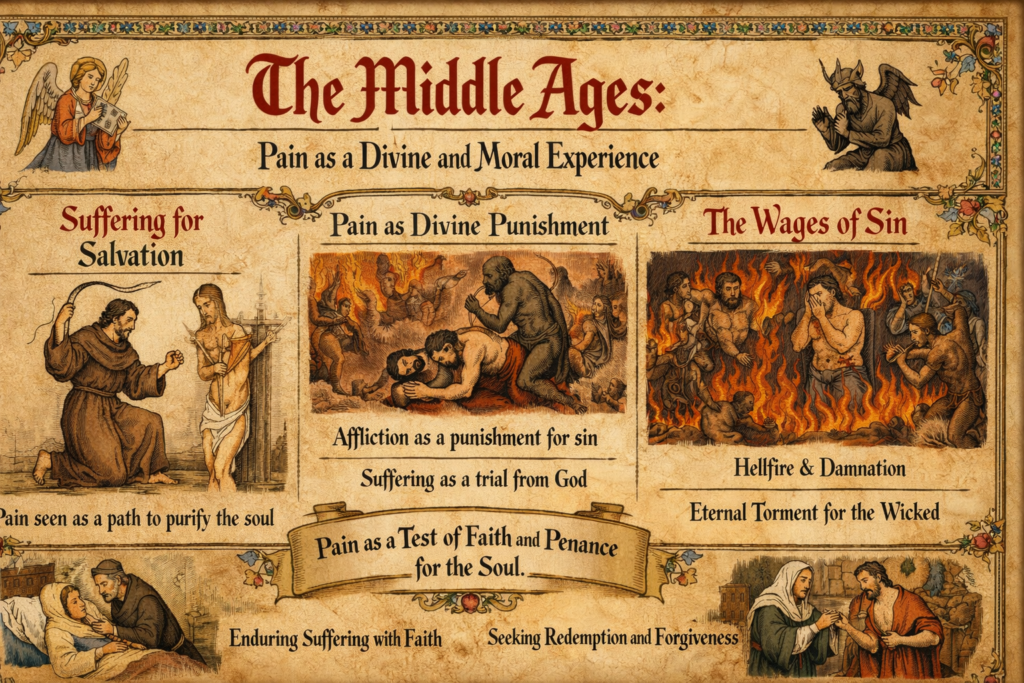
3. The Middle Ages: Pain as a Divine and Moral Experience
During the Middle Ages, roughly spanning the 5th to the 15th century, systematic scientific investigation into pain largely stagnated in Europe, as theological and philosophical frameworks dominated explanations of bodily phenomena. Medical knowledge was heavily influenced by religious doctrine, classical authorities, and humoral theory, leaving little room for experimental inquiry or anatomical exploration. Pain, in this context, was rarely approached as a physiological process alone, but rather as a phenomenon imbued with moral, spiritual, and existential meaning.
An important exception within this period was the work of Avicenna (Ibn Sina, 980–1037), whose Canon of Medicine exerted a lasting influence on both Islamic and European medicine. Avicenna made a notable conceptual advance by identifying pain as a distinct sensory modality, separate from touch, thereby anticipating later sensory theories. Despite this insight, his ideas were embedded in a broader medical and philosophical system that remained largely speculative and non-experimental.
In everyday life, pain was commonly interpreted as originating beyond the physical body. It was frequently understood as divine punishment for sin, a test of faith, or a necessary means of spiritual purification. Suffering could be viewed as a path toward redemption, imitation of Christ’s passion, or preparation for salvation. As a result, enduring pain without complaint was often valorized, while attempts to relieve it could be morally ambiguous or even discouraged.
Therapeutic responses reflected these beliefs. Prayer, confession, pilgrimage, and other religious practices were central to the management of pain, often taking precedence over physical or pharmacological interventions. Although herbal remedies and basic surgical techniques existed, their use was limited, and analgesia was rudimentary. The spiritual interpretation of pain thus shaped both patient expectations and caregiver responses, reinforcing endurance rather than relief as the ideal response to suffering.
This medieval framing of pain profoundly reinforced its moral and existential dimensions. Importantly, these perspectives did not disappear with the advent of modern medicine; traces remain evident today in cultural attitudes toward suffering, stoicism, guilt, and the perceived meaning of pain. Understanding this historical legacy helps explain why pain is still experienced and interpreted not only as a biological signal, but also as a deeply personal and culturally embedded phenomenon.
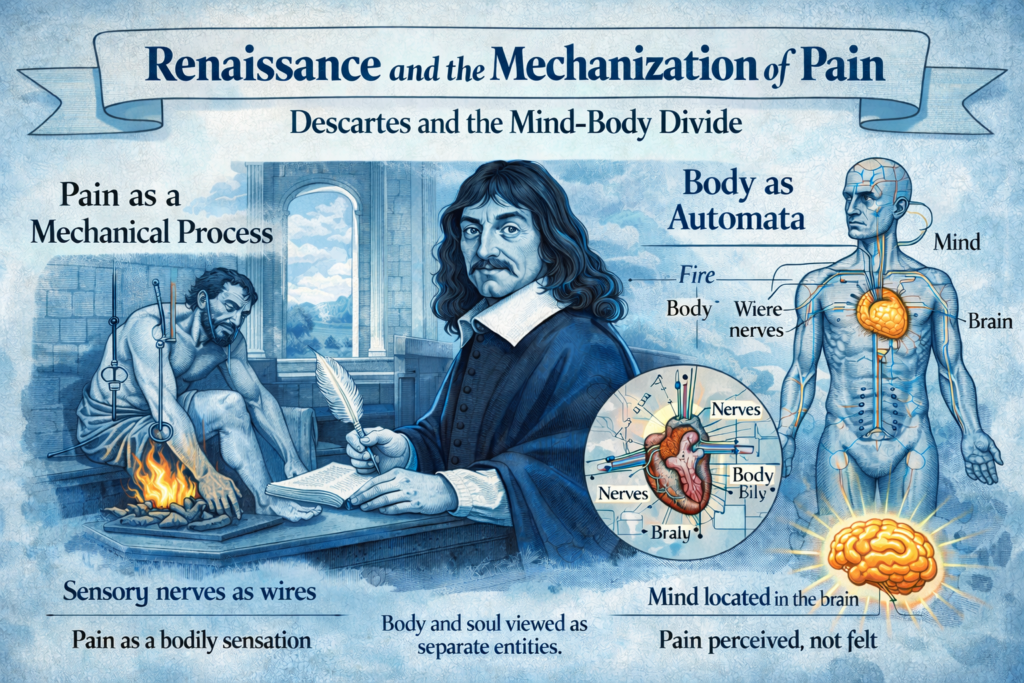
4. Renaissance and the Mechanization of Pain
Descartes and the Mind–Body Divide
A major paradigm shift occurred during the Renaissance with the work of René Descartes. In his Treatise of Man (1664), Descartes conceptualized the human body as a machine. Pain was described as a mechanical disturbance transmitted through nerve pathways to the brain. This model relocated the center of pain perception from the heart to the brain and transformed pain from a spiritual phenomenon into a physiological process.
Descartes’ model introduced the concept of neuronal transmission but excluded psychological influences such as attention, distraction, prior experience, and meaning. Pain was viewed as a direct consequence of tissue injury, an idea that would dominate biomedical thinking for centuries.
https://www.wikiwand.com/en/articles/Treatise_on_Man
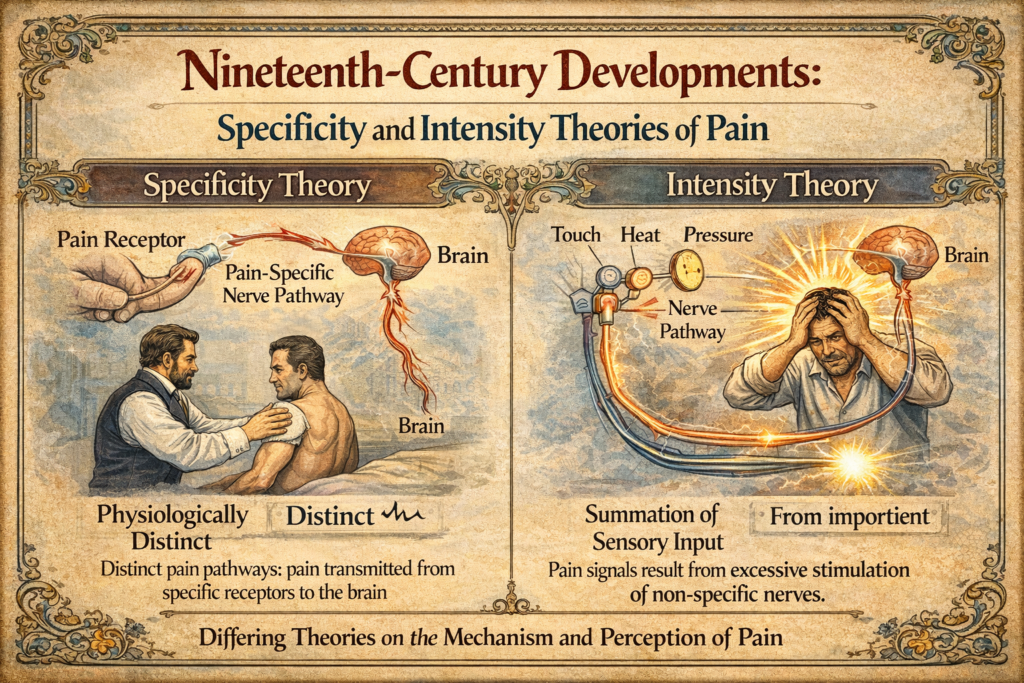
5. Nineteenth-Century Developments: Specificity and Intensity Theories
5.1 Specificity Theory
Advances in anatomy and physiology in the 19th century led to the specificity theory of pain. Charles Bell proposed that sensory receptors were specialized for specific stimuli. Johannes Müller’s doctrine of specific nerve energies suggested that the quality of sensation depended on the nerve pathway activated, not the stimulus itself.
Subsequent discoveries by Pacini, Meissner, Wagner, Schiff, Krause, Blix, and von Frey identified specialized receptors and distinct neural pathways for touch, pressure, temperature, and pain. These findings supported the idea that pain was a distinct sensory modality with dedicated receptors and pathways.
5.2 Intensity Theory
In contrast, psychologists emphasized the intensity theory, proposing that pain resulted from excessive stimulation of nonspecific sensory receptors. Erasmus Darwin and later Wilhelm Erb and Edward Titchener argued that pain emerged when stimulus intensity exceeded a certain threshold. Observations of summation, particularly in patients with neurological conditions such as tabes dorsalis, supported this view.
6. Late 19th and 20th Century Developments
Competition and integration of theories
By the late 19th and early 20th centuries, debate between specificity and intensity theorists intensified. Over time, evidence increasingly favored specificity models, though elements of summation and central processing were acknowledged. Henry Head and von Frey contributed to a synthesis of these ideas, while later concepts introduced the role of interneurons and central modulation.
Gate control theory: a Paradigm shift
The publication of the Gate Control Theory by Melzack and Wall in 1965 marked a revolutionary moment in pain science. The theory proposed that pain signals are modulated at the level of the dorsal horn of the spinal cord by interactions between peripheral input and descending central control. Large-fiber input could “close the gate” to nociceptive signals, while psychological factors such as attention and emotion could influence pain perception. Gate control theory legitimized psychological influences on pain and stimulated extensive research into spinal physiology, descending inhibitory pathways, and pain pharmacology. It also explained why purely surgical approaches to chronic pain often failed.
Emergence of the Biopsychosocial model: Multidimensional nature of pain
In the late 20th century, Engel and Loeser formalized the biopsychosocial model of pain. This framework integrates biological processes (nociception), psychological factors (emotion, cognition), and social context (relationships, culture, work). Pain was no longer equated with tissue damage but understood as a multidimensional experience.
Loeser described pain as comprising multiple components: nociception, sensory perception, affective suffering, cognitive interpretation, and behavioral response. Advances in neuroimaging demonstrated that observing pain in others or focusing attention on pain could modulate neural pain networks, reinforcing the role of context and meaning.
Holistic models and chronic pain
Holistic models emphasize the vicious cycles common in chronic pain: injury leads to maladaptive beliefs, fear, avoidance, deconditioning, social withdrawal, and emotional distress. Family dynamics and failed treatments can further reinforce disability and suffering. These insights have reshaped rehabilitation and interdisciplinary pain management.
Implications for Pain Treatment
The goals of modern pain treatment extend beyond pain reduction alone. They include improving function, enhancing quality of life, fostering adaptive coping, and optimizing social support. Realistic goal-setting and patient-centered care are essential components of effective pain management.